Treating the Foot
As an introduction to the video about treating the foot I want to emphasize certain things that weren’t really emphasized in the video.
It seems that the foot is often neglected except in the common pain conditions like hammertoes, bunions, heel pain and plantar fasciitis.
The image below is the sensory homunculus which represents a proportional representation of body parts on the sensory cortex of the brain. As it is quite evident from that, there are three major areas that have a high representation in the sensory cortex.
Treating each area represented in the homunculus affects different activities of the brain. The feet tend to influence the function of the cerebellum due to do the function of the feet relaying information about ground contact forces. This information processed in the Cerebellum causes the rest the body to do compensatory movements and stay balanced.
Treating the face area lips and tongue tend to influence the limbic area of the brain as the facial areas tend to be involved in emotional expression. Treating the hands tends to affect the cerebral cortex and has a wide effect on many aspects of the body and mind.
I generally treat each of these areas with each patient I see as each area has profound neurological effects on the whole body.
This introduction will concentrate on the importance of treating the feet not only for pain and symptom relief but most importantly to reduce the misinformation sent from the proprioceptive system in the feet to the cerebellum.
The guiding principle for treatment is to mobilize the foot as much as possible, reduce all tensions in the foot and lower extremity, enabling the foot to inform the cerebellum as best as possible as to the ground surface and coordinate balance and moving based on that information.
Ideally, a healthy foot should have these properties:
Consider the ankle perpendicular to the tibia/fibula, i.e. 90 degrees
Ankle dorsiflexion should easily go to 110+ degrees and be smooth without deviation
Ankle plantar flexion 50 degrees
The forefoot should adduct 20 degrees, abduct 10 degrees
Whole foot inversion is not usually restricted occasionally eversion is reduced.
Plantar flexion of the tarsal/cuneiform joints is commonly less in the left foot compared to the right. Also many times, the inferior glide of the tarsals at this joint is reduced so that plantar flexion is affected due to the joint surfaces not being congruent.
The fore foot should evert easily.
The calcaneous tends to be able to invert more than evert which causes a more lateral heel strike.
The first ray should externally and internally rotate equally so that the metatarsal/phalangeal joint moves with the axis parallel to the ground
The first toe metatarsal/phalangeal joint should allow the digit to abduct towards the body’s midline about 10% and the distal toe joint should allow the entire toe to be in line with the metatarsal.
The talocrural joint usually has differences in anterior and posterior draw signs. Stabilizing the foot at the calcaneous, comparisons are made by wrapping the other hand around the lower tibia and fibula checking the joint glide by pulling the tib/fib anterior and pushing posterior. The posterior push maneuver is generally looser and has a different end feel. The difference is due to the constant posterior force of the lower leg while the foot is a fixed position in the stance phase to toe off and over time causing laxity in the restraining ligaments.
.
At the beginning of treating anyone, no matter what the chief complaint is, assess for a short leg and pelvis. Information is here:
Note also that I am using a percussion vibrator at a very low speed. Using this in combination with direct pressure, usually very close to tendon and ligament insertions, enables releases to occur in less than ten seconds, usually with 3-4 seconds.
First check the ability of the ankles to dorsiflex. It should dorsiflex about 20° past perpendicular. If it’s difficult to even get to 90° dorsiflexion this will cause problems in the body above. If it is difficult for the tibia to be perpendicular to the ground the body will be tending to be pushed backwards by the inability to dorsiflex easily. Sometimes there’s a significant difference between the right and left ankle dorsiflexion. The side that has the least ability to dorsiflex will cause tension in the opposite quadratus lumborum muscle. This is due to the inability of the toes to clear the ground going from push off to heel strike. In order to clear the toes the person will lien to the opposite side which will effectively increase the space of ground clearance. If dorsiflexion is reduced reach under the supine patient and palpate the space between the rib cage and the iliac crest to find the quadratus lumborum muscles. After the decreased dorsiflexion is corrected palpate the quadratus lumborum muscles again and one that was previously very tight will be significantly looser.
The muscles that are frequently paid little attention to are the extensor digitorum brevis and the extensor hallicus brevis. Both muscles dorsiflex metatarsal/phalangeal joints. Ideally these joints should plantar flex to around 45°. Often times the tension in these two muscles prevents the proximal phalanx to plantarflex to 0°. Several problems are associated with these muscles being unable to allow plantar flexion to 45°. First is what I will call functional hammer toes. Observing the relaxed foot, the toes are not straight and look to be clawed. This is different than a structural hammertoe foot in that when the toes are passively made to straighten there is no joint blockages to prevent that. In structural hammertoes, typically the proximal inter-phalangeal joint cannot straighten due to problems in the joint itself. The curling of the toes is due to the long toe flexors shortening.
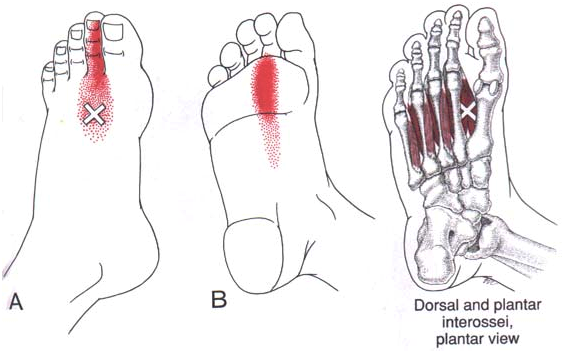
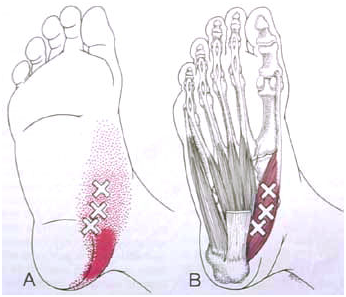
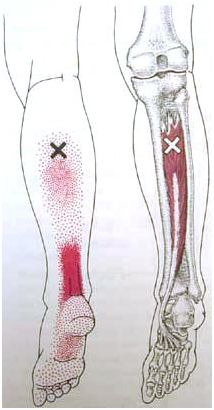
The tight extensor digitorum brevis and extensor Hallicus brevis are the root causes of plantar fasciitis. When these muscles are tight they prevent full plantar flexion of the toes which then causes a significant increase of tension in the muscles of the foot and calf, often times generating multiple trigger points which then refer pain to various portions of the foot. The resulting foot pain is mistakenly named plantar fasciitis. I refer you to the picture below for muscles that refer pain to the foot and Achilles tendon pain.
In my experience treating the extensor digitorum brevis and extensor Hallicus brevis so that the plantarflexion of the metatarsal phalangeal joints is returned to normal, those trigger points resolve and there’s no longer foot pain. Most standard treatments seem to be aimed at stretching the plantar fascia which if you understand its function does not stretch as it serves to transmit forces and stabilize the foot. Stretching the calf muscles is also used, but it’s not really treating the cause of the foot pain which can be relieved by treating the extensor digitorum brevis and extensor Hallicus brevis so that the metatarsal phalangeal joint has full-motion and the muscles of the foot and calf no longer have to strain and work so hard. In my practice, most cases of plantar fasciitis are relieved in about 20 to 30 minutes of treating those two muscles to have them completely release and be relaxed.
The extensor digitorum also inhibits the lumbrical muscles. These little muscles are important in the push-off phase of gait. The lumbricals plantar flex the metatarsal phalangeal joint and extend the inter phalangeal joints, thus making the toes straight when the the foot and toe flexors contract. The correct function of the lumbricals support the maximum force transmitted during push-off.
“A note on using the dowel and hammer technique seen the the video….It should be placed very firmly against the place that is treated. Then tap. If more force is needed don’t hit harder but hit the dowel with a section of the handle closer to the hand holding it.”
The calcaneus or heel bone is another place that generally needs to be corrected in many people. The calcaneus, in many people, inverts much more than it everts. This places the heel strike more laterally on the calcaneus which in turn causes the foot and forefoot to pronate more to get the ball of the big toe in contact with the ground. Increasing calcaneal eversion will then get the heel strike on the mid-calcaneal bone so that the forefoot doesn’t have to travel as much to get the ball of the big toe in contact with the ground. Once the forefoot is treated to increase plantar flexion, eversion and adduction, the ball of the big toe should contact the ground easily to bear weight, without excessive foot pronation.
At 37:25 I refer to constricted connective tissue. Often times the shortened/tight extensor digitorum brevis/hallicus cause the subcutaneous fascia and skin to shorten preventing full plantar flexion of the toes. The individual metatarsal/phalangeal joint capsule tissues may also be shortened and both areas should be treated if needed. At about 40:45, a discussion about the big toe deviating through the movements of plantar to dorsiflexion. To treat the deviation, I hold the toe in the position where it starts to deviate, palpate for the restriction, treat until released, and usually the movement is significantly better. Check internal/ external rotation of the big toe at the metatarsal/ cuneiform joint. It should be equal so that the axis of the metatarsal/phalangeal joint is parallel to the ground.
I sometimes used the terms adduction and abduction not entirely correctly. Spreading the toes apart is abduction but with the big being referenced to the body’s midline can sometimes be labeled adduction
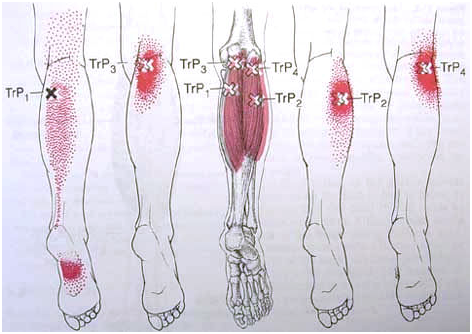
Gastrocnemius
Hallucis muscles

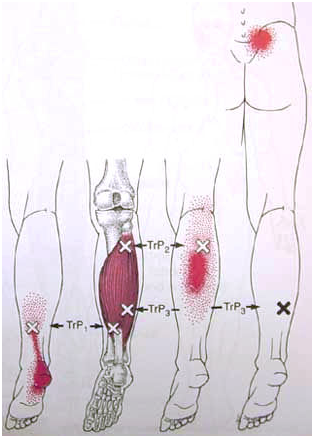
Soleus
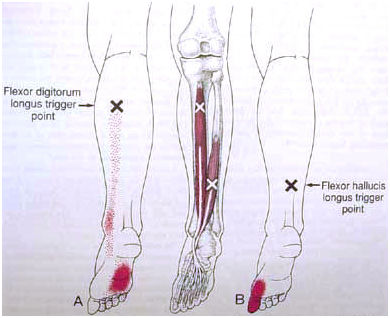
Flexor Digitorum longus
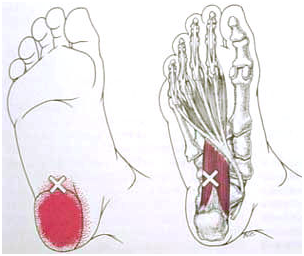
Interossei
Adductor Hallucis
Tibialis Posterior
Quadratus Plantae